Overview
 The Achilles tendon is situated above the heel and forms the lower part of the calf muscles. It is a continuation of the two calf muscles, the gastrocnemius and soleus muscles, and it attaches to the heel bone. It is the strongest tendon in the human body and must withstand great forces. Its function is to transmit the force produced by the calf muscles to lift the heel and produce the push off during walking, running and jumping. The Achilles can produce force of up to seven times body weight. This shows just how much force it has to withstand during sporting activities, such as sprinting, jumping and turning.
The Achilles tendon is situated above the heel and forms the lower part of the calf muscles. It is a continuation of the two calf muscles, the gastrocnemius and soleus muscles, and it attaches to the heel bone. It is the strongest tendon in the human body and must withstand great forces. Its function is to transmit the force produced by the calf muscles to lift the heel and produce the push off during walking, running and jumping. The Achilles can produce force of up to seven times body weight. This shows just how much force it has to withstand during sporting activities, such as sprinting, jumping and turning.
Causes
Ruptured Achilles tendons may result from falling from a height or down a hole. Increasing training intensity abruptly, boosting distance, frequency or duration by more than 10% a week. Failing to stretch before and after exercise. Repetitive training, especially uphill running. Deyhydration, which causes cramping and tightness in the calves. Taking antibiotics. Improper footwear. Explosive movements in competitive sports like basketball, soccer or track & field.
Symptoms
Although it's possible to have no signs or symptoms with an Achilles tendon rupture, most people experience pain, possibly severe, and swelling near your heel. An inability to bend your foot downward or "push off" the injured leg when you walk. An inability to stand up on your toes on the injured leg. A popping or snapping sound when the injury occurs. Seek medical advice immediately if you feel a pop or snap in your heel, especially if you can't walk properly afterward.
Diagnosis
A diagnosis can be made clinically, but an MRI or ultrasound scan can confirm it. On examination, the patient will present with reduced plantarflexion strength, a positive Thompson test and potentially, a palpable gap in the Achilles. The whole length of the tendon should be examined to check for injuries that can occur at the insertion and the musculotendinous junction.
Non Surgical Treatment
Nonsurgical method is generally undertaken in individuals who are old, inactive, and at high-risk for surgery. Other individuals who should not undergo surgery are those who have a wound infection/ulcer around the heel area. A large group of patients who may not be candidates for surgery include those with diabetes, those with poor blood supply to the foot, patients with nerve problems in the foot, and those who may not comply with rehabilitation. Nonsurgical management involves application of a short leg cast to the affected leg, with the ankle in a slightly flexed position. Maintaining the ankle in this position helps appose the tendons and improves healing. The leg is placed in a cast for six to 10 weeks and no movement of the ankle is allowed. Walking is allowed on the cast after a period of four to six weeks. When the cast is removed, a small heel lift is inserted in the shoe to permit better support for the ankle for an additional two to four weeks. Following this, physical therapy is recommended. The advantages of a nonsurgical approach are no risk of a wound infection or breakdown of skin and no risk of nerve injury. The disadvantages of the nonsurgical approach includes a slightly higher risk of Achilles tendon rupture and the surgery is much more complex if indeed a repair is necessary in future. In addition, the recuperative period after the nonsurgical approach is more prolonged.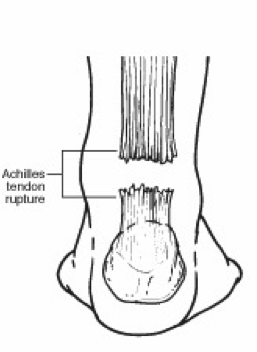
Surgical Treatment
Surgery will involve stitching the two ends of the tendon together, before placing the leg in a cast or brace. The advantage of having an operation is the reduced chance of the rupture reoccurring, however it will involve the risks associated with any surgical procedure, such as infection.
The Achilles tendon is situated above the heel and forms the lower part of the calf muscles. It is a continuation of the two calf muscles, the gastrocnemius and soleus muscles, and it attaches to the heel bone. It is the strongest tendon in the human body and must withstand great forces. Its function is to transmit the force produced by the calf muscles to lift the heel and produce the push off during walking, running and jumping. The Achilles can produce force of up to seven times body weight. This shows just how much force it has to withstand during sporting activities, such as sprinting, jumping and turning.Causes
Ruptured Achilles tendons may result from falling from a height or down a hole. Increasing training intensity abruptly, boosting distance, frequency or duration by more than 10% a week. Failing to stretch before and after exercise. Repetitive training, especially uphill running. Deyhydration, which causes cramping and tightness in the calves. Taking antibiotics. Improper footwear. Explosive movements in competitive sports like basketball, soccer or track & field.
Symptoms
Although it's possible to have no signs or symptoms with an Achilles tendon rupture, most people experience pain, possibly severe, and swelling near your heel. An inability to bend your foot downward or "push off" the injured leg when you walk. An inability to stand up on your toes on the injured leg. A popping or snapping sound when the injury occurs. Seek medical advice immediately if you feel a pop or snap in your heel, especially if you can't walk properly afterward.
Diagnosis
A diagnosis can be made clinically, but an MRI or ultrasound scan can confirm it. On examination, the patient will present with reduced plantarflexion strength, a positive Thompson test and potentially, a palpable gap in the Achilles. The whole length of the tendon should be examined to check for injuries that can occur at the insertion and the musculotendinous junction.
Non Surgical Treatment
Nonsurgical method is generally undertaken in individuals who are old, inactive, and at high-risk for surgery. Other individuals who should not undergo surgery are those who have a wound infection/ulcer around the heel area. A large group of patients who may not be candidates for surgery include those with diabetes, those with poor blood supply to the foot, patients with nerve problems in the foot, and those who may not comply with rehabilitation. Nonsurgical management involves application of a short leg cast to the affected leg, with the ankle in a slightly flexed position. Maintaining the ankle in this position helps appose the tendons and improves healing. The leg is placed in a cast for six to 10 weeks and no movement of the ankle is allowed. Walking is allowed on the cast after a period of four to six weeks. When the cast is removed, a small heel lift is inserted in the shoe to permit better support for the ankle for an additional two to four weeks. Following this, physical therapy is recommended. The advantages of a nonsurgical approach are no risk of a wound infection or breakdown of skin and no risk of nerve injury. The disadvantages of the nonsurgical approach includes a slightly higher risk of Achilles tendon rupture and the surgery is much more complex if indeed a repair is necessary in future. In addition, the recuperative period after the nonsurgical approach is more prolonged.
Surgical Treatment
Surgery will involve stitching the two ends of the tendon together, before placing the leg in a cast or brace. The advantage of having an operation is the reduced chance of the rupture reoccurring, however it will involve the risks associated with any surgical procedure, such as infection.
